Just before new years, the residents asked me to see a patient who had been admitted to the hospital for hiccoughs. When I saw him, the story was a bit more complicated, and included a motor vehicle accident with head trauma 10 years ago, and had been told that he had a hematoma but then had no follow up. He had a left sided daily headache for 2-3 years, pain around (but not inside) the left ear for several days, bleeding from the left ear for one day, and one day of subjective fever within the week prior to admission. At the end of the encounter, they mentioned that he had Hepatitis B and had been treated with interferon for 15 weeks several years ago. His headache was variable, not always in the morning, and didn’t fit migraine or cluster headache patterns either. It had improved with paracetamol, and his hiccoughs (his original presenting complaint) had been present for a week prior to admission, and had improved but not completely resolved over several days with metoclopramide. (He came on Friday and I saw him on Monday or Tuesday.) I think the residents had already decided to do a head CT, and I encouraged them with that plan, explaining that Hiccoughs can come from the brain/nerves or the diaphragm, and I was hopeful that his were from the diaphragm, but his story was worrisome that they might be from the brain.
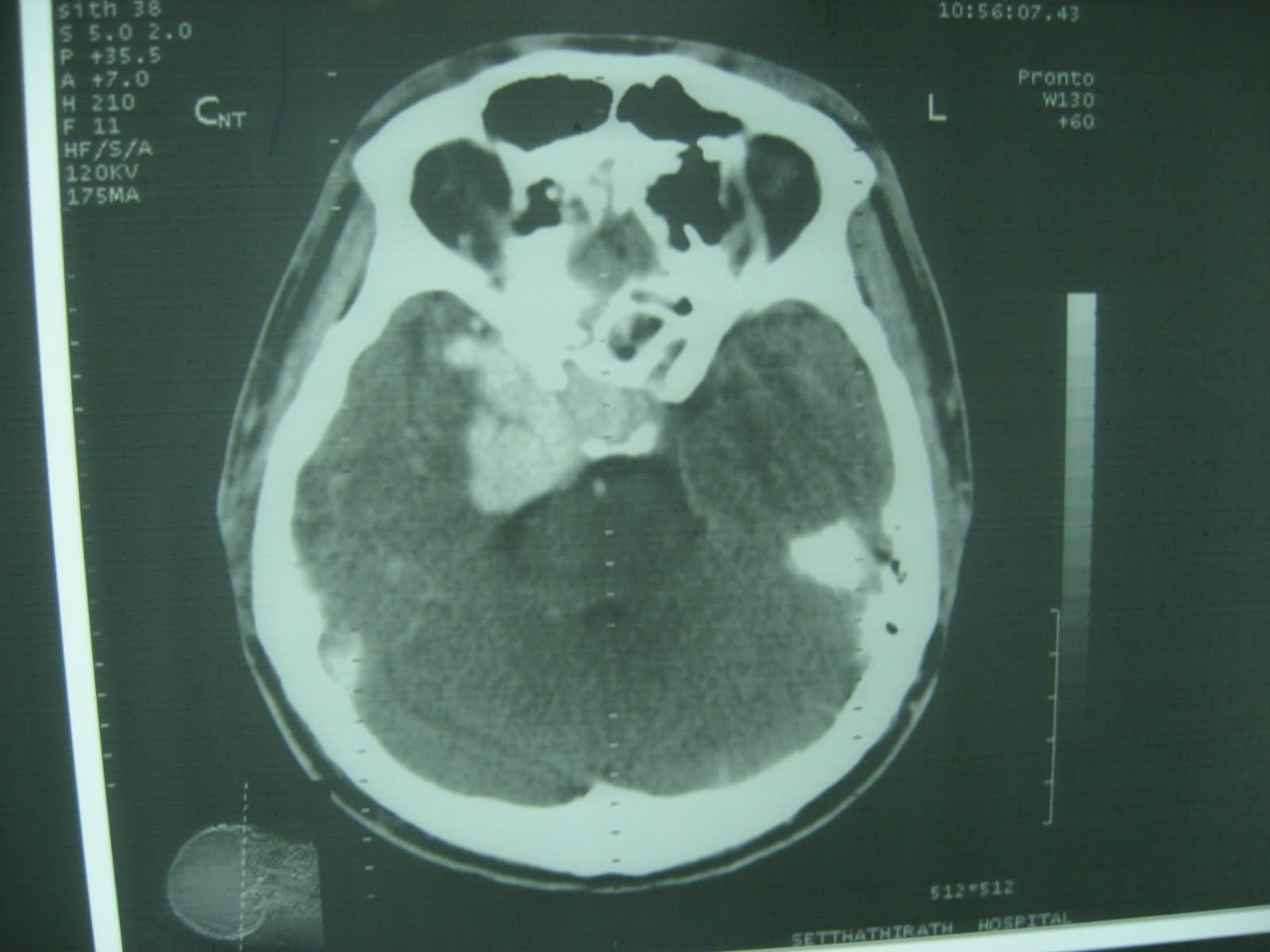
The next day, I was asked to look at his head CT. He had multiple lesions, including an area on the right side that looked like an old stroke or hematoma - mostly empty space where there should have been brain - an 2 spots that light up homogeneously with contrast - one near the left ear, and one on the right, at the very front of the brain near the pituitary gland and optic nerves. And it looked like maybe he had an old fracture in his right sinuses that had not completely healed. The enhancing lesions looked most like tumor - they were very regular - but I was praying for infection (or something else we could treat.) Either way, it was clear he needed an MRI and a neurologist, so the residents sent him home with plans to see Lao’s only neurologist (and a HF internal medicine residency grad) after his MRI in Thailand. A week and a half or so later, he returned to Setta with his MRI read. 11 pages of images in a 5x6 grid. The residents asked me to interpret it for them, because there was no read.
By the 6th or 7th page I was pretty discouraged. I couldn’t tell what kind of lesion the biggest, most worrisome one was, at the R front of the brain. It didn’t look like an abscess or a tumor to me, but I’m also not really trained to read brain MRIs. I’m not a neuro-radiologist, a neurosurgeon, or a neurologist, and while I occasionally look at brain MRIs, I usually do so with a detailed explanation of the results in front of me. I’d like to think I could see acute ischemia or a tumor or parasites on an MRI, but subtle differentiations are certainly beyond me. Fortunately for me, page 9 revealed a possible answer. The malformation lit up with IV contrast too - A LOT - like a blood vessel, not a tumor. Page 11 was the MRA and it clearly showed lots of blood flowing to the area and contrast filling the veins much quicker on the R. Maybe it wasn’t tumor but a crazy big aneurism or AVM? Would that be good or bad for my patient in a country with one neurologist and limited neurosurgeons, maybe none who specialize in vascular problems? I decided it was better than tumor, and explained my theory to the residents with multiple disclaimers about my lack of qualification to interpret MRIs, and they agreed to send the images on to the neurologist. The next day we got the official read from Thailand - he did, in fact, have a large abnormal vascular malformation in the R parasellar region. The neurologist tells me he and the surgeons will discus whether it can be repaired in Lao or he needs to go to Thailand. (And hopefully someone has figured out what the abnormality is on the Left side of the brain -that one wasn’t in the read we got.) But I left the hospital that day feeling proud of my deductive reasoning skills, if not my MRI reading ones. And while the patient isn’t “fixed” yet, he did have appropriate diagnostic testing in a timely fashion, and is being directed to the people who can decide when and how to fix him. :) That’s often as close as we get to a win in Laos.
 At around the same time, a 15 year old girl was admitted to the inpatient medicine wards. It’s ok for my residents to take care of kids sometimes, because when they go home to their districts they may be the only competent doctor, and they will certainly be expected to care for everyone who shows up in the ER when they’re on call. However, I really do not feel qualified supervising them in the care of pediatric patients, particularly here in Lao; not only am I not trained in peds in america, I know nothing about the diseases that are more common here, or specific to SE asia, in children. However, the residents reported that they had asked the pediatricians if they’d like to take over the care of the patient and they weren’t interested. And she was looking pretty sick. She had had more than 3 months of abdominal pain, diarrhea, and weight loss. She now had anasarca and had had an albumin that was too low to measure (less than 2.7) on a check several months ago and again on admission. My resident really wanted it to be nephrotic syndrome (which is pretty common in SE asia) but she had multiple UAs that showed no protein. He was worried that it might be Capillaria philippinensis. This did not make a little light bulb appear over my head. Maybe we talked about it in global health class, but if we did I wasn’t remembering it. However, she did have Opisthorchis, a parasite that you get from eating raw fish, in her stool, and we determined that she had not been treated for this during her previous stay in the hospital. (No one had asked this, or reviewed the chart to see if treatment was prescribed.) So we agreed that we would repeat the few labs that hadn’t been ordered in the ER and treat the parasite we knew she had.
At around the same time, a 15 year old girl was admitted to the inpatient medicine wards. It’s ok for my residents to take care of kids sometimes, because when they go home to their districts they may be the only competent doctor, and they will certainly be expected to care for everyone who shows up in the ER when they’re on call. However, I really do not feel qualified supervising them in the care of pediatric patients, particularly here in Lao; not only am I not trained in peds in america, I know nothing about the diseases that are more common here, or specific to SE asia, in children. However, the residents reported that they had asked the pediatricians if they’d like to take over the care of the patient and they weren’t interested. And she was looking pretty sick. She had had more than 3 months of abdominal pain, diarrhea, and weight loss. She now had anasarca and had had an albumin that was too low to measure (less than 2.7) on a check several months ago and again on admission. My resident really wanted it to be nephrotic syndrome (which is pretty common in SE asia) but she had multiple UAs that showed no protein. He was worried that it might be Capillaria philippinensis. This did not make a little light bulb appear over my head. Maybe we talked about it in global health class, but if we did I wasn’t remembering it. However, she did have Opisthorchis, a parasite that you get from eating raw fish, in her stool, and we determined that she had not been treated for this during her previous stay in the hospital. (No one had asked this, or reviewed the chart to see if treatment was prescribed.) So we agreed that we would repeat the few labs that hadn’t been ordered in the ER and treat the parasite we knew she had. I went home and read about Capillaria philippinensis. It turns out that you get it the same way - eating raw fish - and it is one of the rare parasites that will actually kill you without treatment. It causes chronic diarrhea, abdominal pain, and protein loosing enteropathy. (All of the symptoms our patient had.) And it can be hard to find on stool exams. And almost all patients who have it have other parasites as well. And there have been cases in Lao. All of this was adding up to make me very worried about this patient. I e-mailed our beloved ID doc who agreed that the story was worrisome but suggested we also consider beri-beri (thiamine deficiency.) Another condition I have never actually seen in America. I reported this back to the residents. We discussed how she didn’t have the parasites on another stool exam, but we knew she had one parasite, which made others more likely. We discussed how clinically, the picture was compatible, and how these particular parasites can be hard to find on stool exam. We discussed how not treating capillariasis is deadly. We discussed the risk / benefit of possibly giving anti-parasite drugs she doesn’t need (side effects/toxicities) vs. the risk of not treating the infection (death.) The residents reported that they agreed with me but the teachers said they couldn’t give albendazole, the medicine for capillariasis. They did give some thiamine.
Over the next week, her anasarca improved and her fatigue improved a bit. She looked more like a chronically ill patient, but not one on the verge of death, the way she had the first day or two. She started eating a little, sitting up, and interacting with the doctors. Maybe she had just had thiamine deficiency, but probably not, because thiamine deficiency doesn’t cause abdominal pain, and it usually does cause other symptoms / exam findings that she did not have. I had the same discussion about likelihood of infection (Unknown, but certainly non-zero), and risk/benefit of treatment vs not treating several more times with the residents, and one time with the IM teachers and ID team there. They all sort of nodded their heads, but every day she still hadn’t been put on albendazole. This monday, I came in to the hospital and she was gone. She was discharged over the weekend, having never been given albendazole. The residents reported they would have liked to give it, but the teachers kept saying no. I can only hope that if she gets worse again (which she will do if she has untreated infection with this particular parasite) she comes back to Setta, either to the IM ward where I can try again, or to the peds ward where the docs can at least look at all the recent notes saying ?capillariasis and consider it as a diagnosis. But I feel like we failed a young woman with a lot of potential life left ahead of her, and that is discouraging.

No comments:
Post a Comment